
With no true endgame or advance directive, Tom Brady’s legacy as an NFL superstar and family man remains nebulous.
Is his recent retirement from playing football officially ‘the end? Will he entertain offers to stay alive and play yet another year? With being at the 45-year-old “yard line” and facing the goalpost at the end of the field, what’s his endgame for the next year?
When do the false promises end and the final wishes begin?
Like Tom Brady, most seniors do not appear to have a ready endgame. The 30 percent of seniors who have advance directives or game strategies are often caught off guard during the rushing game that occurs in emergency rooms. 1 out of 12 seniors over age 80 will die within one month of their last ER visit.
Imagine how quickly a quarterback gets sacked while following the coach’s orders and listening to adoring family members cheering from the sidelines. Seniors and Tom Brady both have options that could allow them to play another year. When’s “enough” enough? How do seniors protect themselves from the inherent risks of pain and suffering by “playing all out?”
The age-old debate between quantity and quality, number of years and quality of life is decided by advance directives that determine the endgame. The purpose of an endgame becomes a choice between two slogans: “Just Do It unconsciously” OR “Do No Harm consciously.”
Many seniors dream about scoring a touchdown by reaching 100 years old. Some are satisfied with kicking a field goal within the 35-yard line after age 65. Some pray for a Hail Mary pass in hopes of reaching the end zone with an advanced illness.
The idea of seniors kicking a field goal after three downs might be seen as scoring points or giving up, ending on a high note versus losing in the end. Understandably, the odds of winning a Super Bowl decrease after age 40, and reaching the end zone of 100 years old is unlikely given that life expectancy is age 80.
If seniors begin Medicare enrollment with the end in mind and hindsight is 20/20, completing an advance directive with Medicare enrollment provides a clear vision for the endgame. After the third down of medical setbacks with advanced illness management, seniors have three choices for the next year:
Medicare Advance Directive A: Go for another first down with inpatient hospitalization
Medicare Advance Directive B: Kick the field goal and receive home care
Medicare Advance Directive C: Say a Hail Mary that’s answered with palliative services
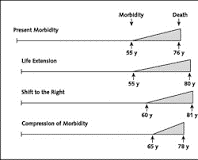
While Directive A extends life, Directives B and C reduce pain and suffering during the final years of life. The Compression of Morbidity Theory, proposed by Dr. James F. Fries at Stanford in 1980, suggests individuals look at the overall trajectory of life and become proactive in staving off advanced illness, then seize the moment at the time of diagnosis by withholding treatment.
If the best way to combat the medical business model of life extension is with an advance directive, then Medicare might advocate for the best interest of seniors by having them complete advance directives with enrollment. Medicare Advance Directives might apply the Compression of Morbidity Theory.
The idea of the Compression of Morbidity Theory is to advance the ball down the field of life until a serious illness leaves us in a do-or-die situation. Those who “do” extend life with Directive A often prolong suffering to the end. Those who “die” peacefully with Directive B experience a new lease on life by kicking a field goal and retiring. Directive C is for those who still want the choice between doing and dying for the next year.
If hindsight is 20/20 and foresight is 50/50, consider the ultimate choice becomes leaving everything on the field with a running game based on fear OR throwing caution to the wind by punting or passing the ball through faith.
If seniors begin Medicare enrollment with foresight being 50/50, they have an equal chance of choosing between Advance Directive A and Advance Directive B, entitlement vs. empowerment. Those who feel entitled rely on teammates to stay in the game. Those who are empowered will do for themselves and retire from the game. Advance Directive C affords a timeout for those who are torn between entitlement and empowerment.
Tom Brady’s choice to extend his NFL career risked dying in vain over resting in peace this past season. His decision reminds us of the wise adage to quit while we’re ahead and compress morbidity. It’s also notable that maximizing his gains cost him the heartbreak of those closest to him.
In the end, we might list priorities to stay alive, live at home, and enjoy family. More important than ending my way (living at home) or Brady’s way (staying alive) is doing what you say you’ll do with integrity. While Directive A asserts staying alive and Directive B enlists living at home, Directive C favors enjoying family.
Inherent dignity exists within each advance directive, but living and dying with dignity is realized through personal integrity . . . declaring and realizing final wishes as definitive and sacred. Tom Brady will be remembered dearly but not likely as a man of integrity. Do we follow his endgame of Directive A, or strive for our own personal best by compressing morbidity and choosing Directive B or C during Medicare enrollment?
Leave a Reply